Levobupivacaine should be administered only by, or under the supervision of, a clinician having the necessary training and experience.
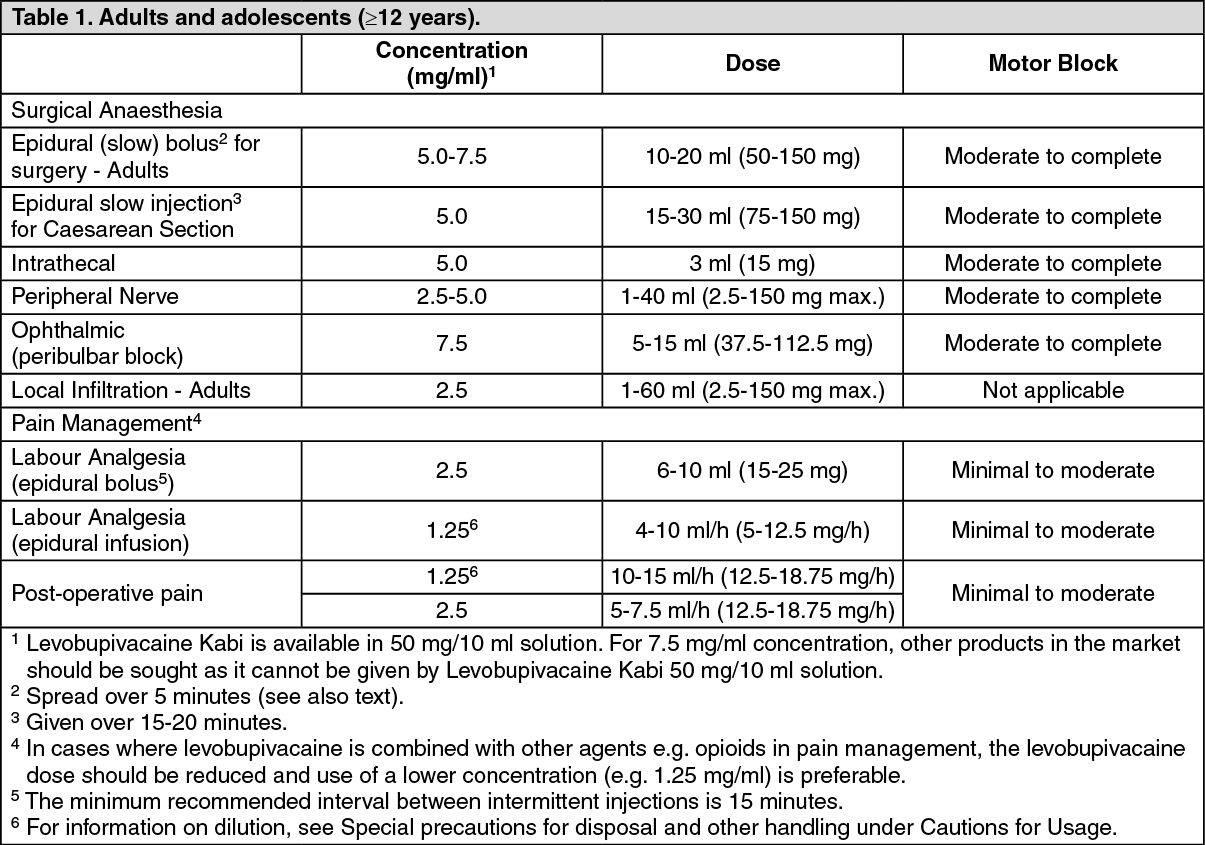
Posology: The following tables are guides to dosage for the more commonly used blocks. For analgesia (e.g. epidural administration for pain management), the lower concentrations and doses are recommended. Where profound or prolonged anaesthesia is required with dense motor block (e.g. epidural or peribulbar block), the higher concentrations may be used. Careful aspiration before and during injection is recommended to prevent intravascular injection.
There is limited safety experience with levobupivacaine therapy for periods exceeding 24 hours. In order to minimise the risk for severe neurological complications, the patient and the duration of administration of levobupivacaine should be closely monitored (see Precautions).
Maximum dose: The maximum dosage must be determined by evaluating the size and physical status of the patient, together with the concentration of the agent and the area and route of administration. Individual variation in onset and duration of block does occur. Experience from clinical studies shows onset of sensory block adequate for surgery in 10-15 minutes following epidural administration, with a time to regression in the range of 6-9 hours.
The recommended maximum single dose is 150 mg. Where sustained motor and sensory block are required for a prolonged procedure, additional doses may be required. The maximum recommended dose during a 24 hour period is 400 mg. For post-operative pain management, the dose should not exceed 18.75 mg/hour.
Obstetrics: For caesarean section, higher concentrations than the 5.0 mg/ml solution should not be used (see Contraindications). The maximum recommended dose is 150 mg.
For labour analgesia by epidural infusion, the dose should not exceed 12.5 mg/hour.
Paediatric population: In children (<12 years), the maximum recommended dose for analgesia (ilioinguinal/iliohypogastric blocks) is 1.25 mg/kg/side.
The maximum dosage should be adjusted according to the size, body constitution and physical status of the patient/child.
The safety and efficacy of levobupivacaine in children for other indications have not been established.
Special populations: Debilitated, elderly or acutely ill patients should be given reduced doses of levobupivacaine commensurate with their physical status.
In the management of post-operative pain, the dose given during surgery must be taken into account.
There are no relevant data in patients with hepatic impairment (see Precautions and Pharmacology: Pharmacokinetics under Actions).
Table of Doses: See Tables 1 and 2.
 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Method of administration:
Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
Method of administration: Levobupivacaine Kabi is indicated for epidural use, intrathecal use, perineural use (peripheral nerve blocks) and for infiltration (including peribulbar use) (see Tables 1 and 2).
Aspiration should be repeated before and during administration of a bolus dose, which should be injected slowly and in incremental doses, at a rate of 7.5-30 mg/min, while closely observing the patient's vital functions and maintaining verbal contact.
If toxic symptoms occur, the injection should be stopped immediately.
For instructions on dilution of the medicinal product before administration, see Special precautions for disposal and other handling under Cautions for Usage.


 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image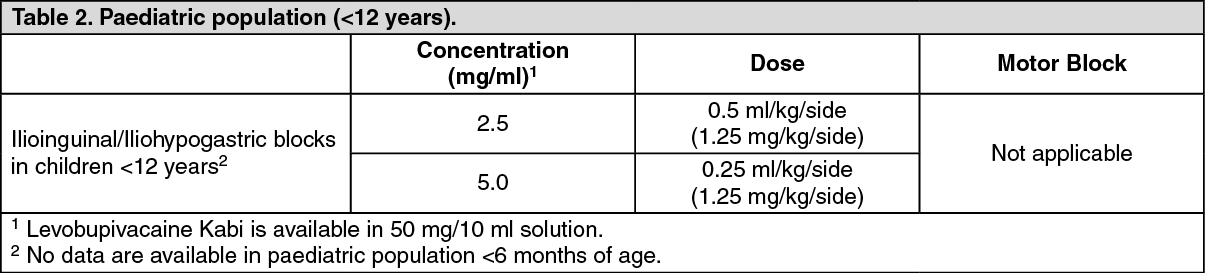 Click on icon to see table/diagram/image
Click on icon to see table/diagram/image Click on icon to see table/diagram/image
Click on icon to see table/diagram/image
 Sign Out
Sign Out